2022. 11. 4. 00:20ㆍ카테고리 없음
안녕하세요! 헬씨부입니다~

오늘은 ' 간의 양성 신생물(Benign neoplasm of the liver) '에 대해 알아보고 정리하겠습니다!
간의 양성 신생물
[Benign neoplasm of the liver]
정의
간의 양성 신생물은 간에 발생한 양성 종양을 말합니다. 다음과 같은 종류가 있습니다.
① 간혈관종
가장 흔한 양성 신생물(종양)로, 혈관이 뭉쳐서 생깁니다. 30~50대 여성에게서 잘 발견됩니다. 원인은 알려지지 않았습니다. 대부분 증상이 없지만, 복통 혹은 복부 불편감이 있을 수 있고, 조기 포만감, 오심, 구토가 있을 수 있습니다. 혈관종이 복부의 장기를 누르거나 밀어서 증상을 유발할 수도 있습니다. 간혹 출혈이나 혈전 등이 발생합니다. 아주 드물지만 혈관종의 지름이 10cm가 넘으면 복강 내로 파열되어 복강혈이 발생하는 경우도 있습니다. 악성으로 변하지 않지만, 간암 등 다른 종양과 혼동을 줄 수 있습니다.
② 간낭종
물혹이라고 부르는 양성 신생물로, 치료할 필요는 없습니다. 40~60대 여성에게 잘 생깁니다. 보통은 1cm 이하의 작은 크기지만 드물게 10cm 이상 큰 낭종이 발견되기도 합니다. 큰 간낭종은 복부에 불쾌감을 줄 수 있고, 낭종에 출혈이나 감염이 생기면 통증이나 열이 날 수도 있습니다. 선천적인 이유로 간에 다양한 크기의 물혹이 여러 개 생기기도 하는데 이를 다발성 간낭종이라고 합니다. 신장과 췌장에도 물혹이 함께 생길 수 있습니다.
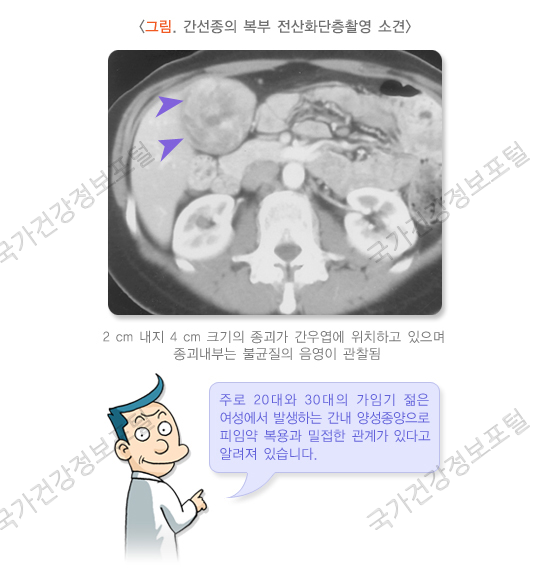
③ 간선종
먹는 피임약과 관련이 있는 양성 신생물로, 피임약을 오래 먹거나 고용량 호르몬제를 복용하면 생길 수 있습니다. 30세 이상의 여성에게서 잘 발견됩니다. 간의 우엽에 주로 발생하고 다발성인 경우도 있습니다. 경구용 피임제를 복용하고 있으면 이를 중단하고, 간선종의 크기가 8~9cm 이상이거나 간 표면에 인접해 있으며 절제할 수 있으면 수술을 시행합니다. 크기가 작을 때는 별다른 증상이 없지만, 종양 내로 출혈이 있거나 커지면 통증이 있을 수 있습니다. 직경이 10cm 이상이거나 다발성인 경우 악성으로 진행될 가능성이 10% 정도 있습니다. 파열 가능성이 있으므로 임신은 피해야 합니다.
④ 국소성 결절성 과증식(FNH)
간의 우엽에 생기는 과형성의 종괴로, 섬유성 핵과 돌기를 가지고 있습니다. 섬유성 돌기에는 비정상적인 간세포와 담도 상피세포, 쿠퍼 세포, 염증 세포들이 있습니다. 간세포 선종과 달리 경구용 피임제와 무관하며 드물게 출혈이나 괴사가 나타납니다. 경구용 피임제를 복용하는 경우 출혈의 위험성이 증가합니다. 증상이 있는 경우 수술을 시행합니다.
⑤ 결절성 재생성 과증식
간문맥 주변의 간세포 증식과 주변부의 위축으로 생긴 다발성 결절입니다. 간경변증이 없는 경우 악성 질환이나 연체 조직 질환 등과 관련이 있을 수 있습니다. 가장 흔한 증상은 문맥 고혈압입니다.
원인
경구 피임약을 사용하는 것이 간선종의 대표적인 위험인자입니다.
간 양성 신생물은 특별한 원인 없이 생기는 경우가 많습니다. 대부분 30~60대의 여성에게서 주로 확인됩니다. 간선종의 경우 장기간의 피임약을 복용하거나, 고용량의 호르몬을 복용하는 경우에 발생할 가능성이 높습니다.
증상
증상이 없는 경우가 흔하고 우상복부 통증을 유발하거나, 복부에서 종괴가 만져지는 경우도 있습니다. 드물게 종괴 파열 및 출혈로 인한 심한 복통, 복강 내 출혈 및 출혈성 쇼크 등의 심각한 합병증을 동반하기도 합니다. 파열된 종괴는 보통 크기가 큰 단일 종괴이며, 파열은 경구용 피임약과 연관된 경우에 가장 흔합니다.
양성 신생물은 5cm 이하일 경우 대부분 증상이 없습니다. 이보다 크기가 큰 경우에는 주위 장기 압박, 복통, 팽만감, 오심, 구토 등의 증세를 보일 수 있습니다.
진단/검사
간 초음파 검사로 0.5cm의 작은 신생물(종양)도 찾아낼 수 있습니다. 조영제를 사용하는 CT 검사를 시행하면 간 초음파보다 더 명확하게 양성 종양인지 악성 종양(간암)인지 구별할 수 있습니다. MRI 검사는 일반 CT 검사로는 잘 확인되지 않는 1cm 이하의 작은 종양을 진단하는 데 유리하며, 혈관종을 더 정확하게 구별해 냅니다. 간동맥 조영술은 혈관에 약물을 주사하면서 X선을 찍어 간의 혈관 모양을 보는 검사로, CT와 MRI에서도 확진하기 힘든 경우 등에 한하여 선택적으로 시행합니다.
주로 간 우엽에 단발성으로 발견되나, 간혹 다발성으로 생기기도 하며 직경이 10cm 이상의 거대한 종괴로 발견되기도 합니다. 복부 초음파 검사, 전산화단층촬영, 자기공명영상, 간동맥조영술 및 핵의학 검사(간주사) 등 영상의학 검사로 진단에 도움을 받을 수 있으나 확진을 위해서는 조직검사가 필요합니다.
치료
간의 양성 신생물은 대부분 수술 치료가 필요하지 않습니다. 다만 양성 신생물과 악성 종양의 구분이 어렵거나, 양성 신생물이지만 크기가 커서 소화기 증상이나 통증을 유발할 때, 혹은 파열의 가능성이 있을 때 수술 치료를 시행합니다.
간선종은 파열의 위험성이 높고 악성화될 수 있음으로 가능하다면 수술적 절제를 하는 것이 필요합니다. 크기가 크거나 간 표면에 가까이 위치해 있어 출혈이나 파열 등의 합병증이 발생할 가능성이 있는 경우, 임신 예정인 경우, 악성인지 양성인지 구별이 힘든 경우에는 수술적 절제가 치료의 원칙입니다. 절제 여부와 상관없이 경구용 피임약은 복용하지 말아야 하며 절제하지 않은 경우에 임신은 피해야 합니다.
경과/합병증
양성 신생물의 종류에 따라 경과 및 합병증이 다릅니다. 다만 간선종의 경우 크기가 커지면 악성으로 진행할 가능성이 있습니다.
문제
A 28-year-old woman presents for a routine health visit. She reports a history of epigastric pain and occasional nausea for 1 week. She denies any history of weight loss, changes in bowel habits, or nausea. Her medical history is unremarkable. She takes an oral contraceptive pill and a multivitamin every day. A physical examination is unremarkable. Liver function tests are within normal limits. A right upper quadrant ultrasound reveals a single 4-cm hypervascular lesion with well-defined margins in the right hepatic lobe. What is the most appropriate next step in the management of this patient’s condition?
|
|
Explanation:
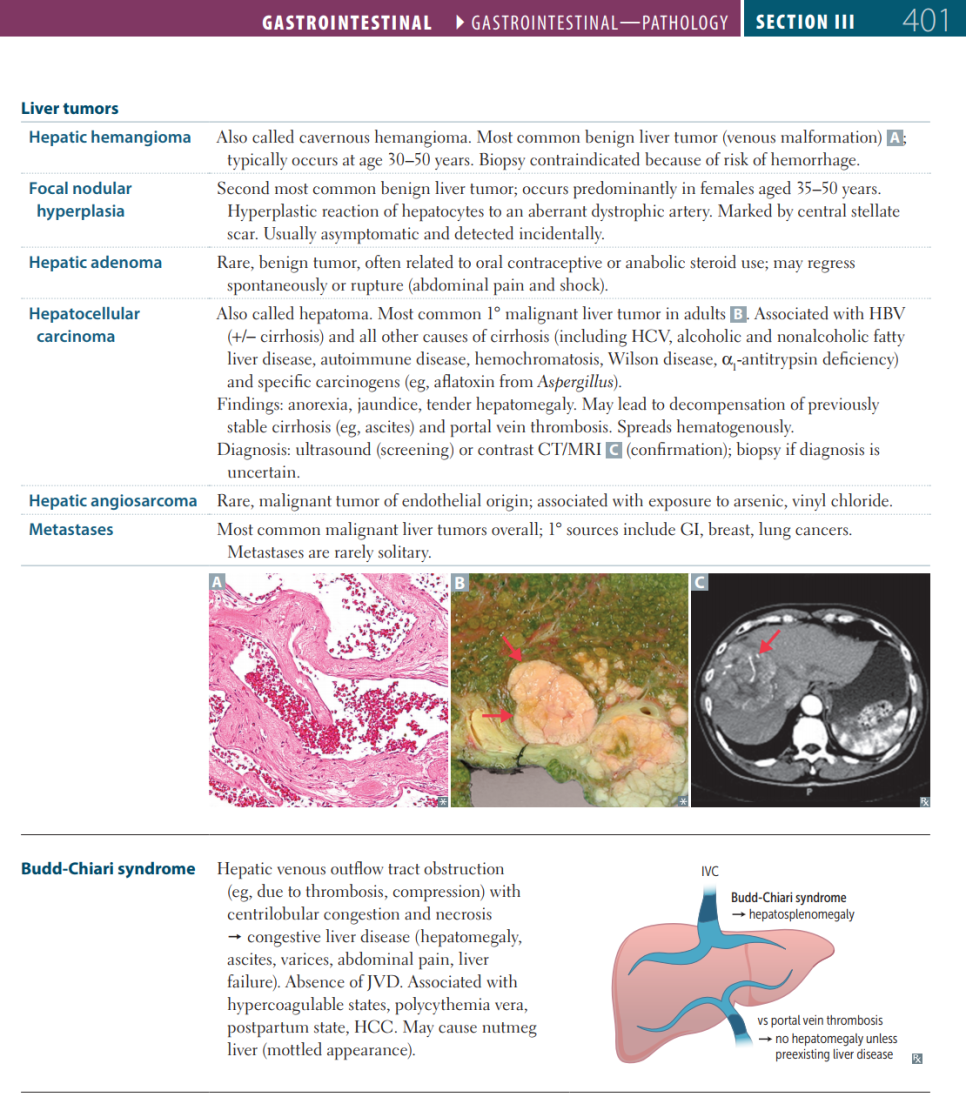
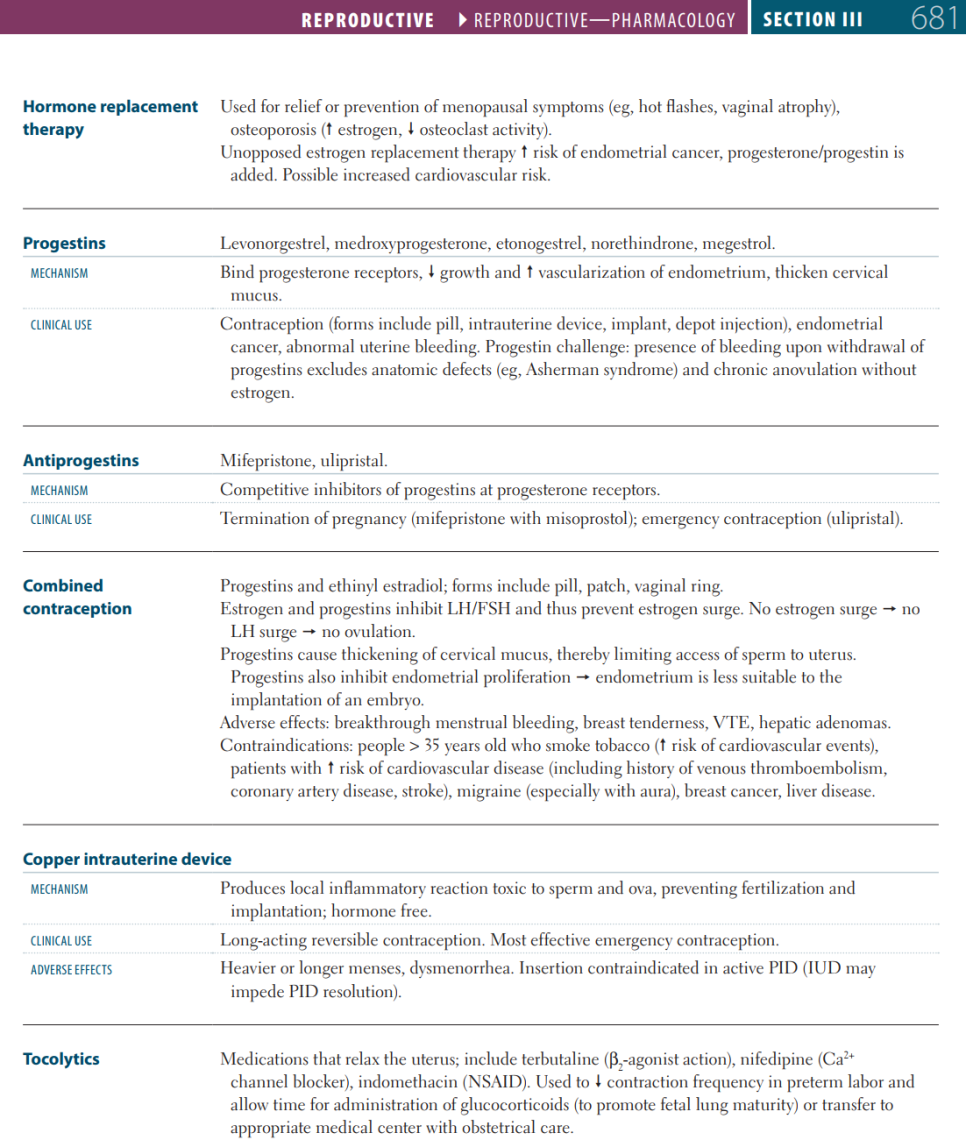
Correct answer A: Hepatic adenomas, also known as hepatocellular adenomas (HCAs), are rare benign solid liver lesions. They typically reproductive-age women using estrogen-containing medications such as combined oral contraceptive pills. They are also associated with anabolic steroid use. Glycogen storage diseases and familial adenomatous polyposis are associated with an increased risk of developing hepatic adenomas. Obesity, metabolic syndrome, and increased alcohol intake are also risk factors, especially in men. HCAs are usually solitary lesions with well-circumscribed margins, ranging in size from a few millimeters to several centimeters; they may be pedunculated when they are subcapsular. They are often located in the right lobe of the liver and are soft and smooth with a pale brown appearance compared to the darker normal hepatic parenchyma. They are usually asymptomatic. The most common symptom is abdominal pain that is episodic and localized to the epigastrium/right upper quadrant. The pain may be due to an enlarged liver, bleeding into the lesion, or necrosis. Hemorrhage can easily occur because a prominent arterial system supplies the hepatic sinusoids and the adenoma has no fibrous capsule. Larger ruptures are associated with sudden severe pain, often with abundant intraperitoneal bleeding, marked hypotension, and death in ~ 20% of cases if not identified and treated emergently. There are 3 subtypes of HCA, based on their genotype and phenotype: ● HCA with hepatocyte nuclear factor (HNF)-1 alpha mutation: account for 35-50%; almost always in women, histologically, they show diffuse steatosis ● Inflammatory HCA: account for 40–55%; mostly in women; histologically, they show inflammatory infiltrates, sinusoidal dilation, tortuous blood vessels, and hemorrhage. ● HCA with beta-catenin activation: account for 10–15%; mostly in men who take or have taken androgens; histologically they show cellular atypia and cholestasis. This type is associated with a much higher risk for malignant transformation (to hepatocellular carcinoma). Histologically, except for inflammatory HCA, which has biliary ductules, the other 2 types of HCAs do not show normal hepatic architecture (i.e., no portal tracts or bile ductules), which helps distinguish HCA from focal nodular hyperplasia, which results from a hyperplastic (regenerative) reaction to an aberrant dystrophic artery. Regarding management of HCAs:
Option B: Radiofrequency ablation has no clear role in the treatment of hepatic adenomas. Option C: CT-guided biopsy is not recommended as the lesions are benign and there is a possibility of hemorrhage during the biopsy. Option D: Referral for surgical excision may be the next step in the management if the mass continues to enlarge after the oral contraceptive pills are discontinued. Option E: Observation is not recommended because this patient is symptomatic. Observation is reasonable in patients who have asymptomatic lesions without pain. Learning objective: Hepatocellular adenomas (HCAs) are rare benign liver tumors that can be hormone-induced. The tumors are usually solitary and asymptomatic. However, they may be associated with symptoms ranging from mild pain to life-threatening hemorrhage if rupture occurs. HCAs are most often associated with the use of estrogen-containing medications such as oral contraceptive pills. Discontinuing the use of oral contraceptive pills is the first step in the management of these patients. Lesions > 5 cm should be resected. |
|
Related Videos:
|
|
Book References:
First Aid for the USMLE Step 1 (2022, 32nd ed): 401, 681
First Aid for the USMLE Step 1 (2021, 31st ed): 402, 681
First Aid for the USMLE Step 1 (2020, 30th ed): 392
First Aid for the USMLE Step 1 (2019, 29th ed): 386
First Aid for the USMLE Step 1 (2018, 28th ed): 386
First Aid for the USMLE Step 1 (2017, 27th ed): 375
|
참고자료

오늘은 여기까지 정리하겠습니다!
감사합니다!
